Glomerular Diseases
Many diseases affect kidney function by attacking the glomeruli, the tiny units within the kidney where blood is cleaned. Glomerular diseases include many conditions with a variety of genetic and environmental causes, but they fall into two major categories:
- Glomerulonephritis (gloh-MEHR-yoo-loh-nef-RY-tis) describes the inflammation of the membrane tissue in the kidney that serves as a filter, separating wastes and extra fluid from the blood.
- Glomerulosclerosis (gloh-MEHR-yoo-loh-skleh-ROH-sis) describes the scarring or hardening of the tiny blood vessels within the kidney.
Although glomerulonephritis and glomerulosclerosis have different causes, they can both lead to kidney failure.
What are the kidneys and what do they do?
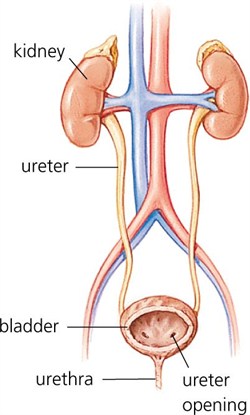
The two kidneys are bean-shaped organs located just below the rib cage, one on each side of the spine. Everyday, the two kidneys filter about 120 to 150 quarts of blood to produce about 1 to 2 quarts of urine, composed of wastes and extra fluid.
Blood enters the kidneys through arteries that branch inside the kidneys into tiny clusters of looping blood vessels. Each cluster is called a glomerulus, which comes from the Greek word meaning filter. The plural form of the word is glomeruli. There are approximately 1 million glomeruli, or filters, in each kidney. The glomerulus is attached to the opening of a small fluid-collecting tube called a tubule. Blood is filtered in the glomerulus, and extra fluid and wastes pass into the tubule and become urine. Eventually, the urine drains from the kidneys into the bladder through larger tubes called ureters.

Each glomerulus-and-tubule unit is called a nephron. Each kidney is composed of about 1 million nephrons. In healthy nephrons, the glomerular membrane that separates the blood vessel from the tubule allows waste products and extra water to pass into the tubule while keeping blood cells and protein in the bloodstream.
[Top]
How do glomerular diseases interfere with kidney function?
Glomerular diseases damage the glomeruli, letting protein and sometimes red blood cells leak into the urine. Sometimes a glomerular disease also interferes with the clearance of waste products by the kidney, so they begin to build up in the blood. Furthermore, loss of blood proteins like albumin in the urine can result in a fall in their level in the bloodstream. In normal blood, albumin acts like a sponge, drawing extra fluid from the body into the bloodstream, where it remains until the kidneys remove it. But when albumin leaks into the urine, the blood loses its capacity to absorb extra fluid from the body. Fluid can accumulate outside the circulatory system in the face, hands, feet, or ankles and cause swelling.
[Top]
What are the symptoms of glomerular disease?
The signs and symptoms of glomerular disease include
- albuminuria: large amounts of protein in the urine
- hematuria: blood in the urine
- reduced glomerular filtration rate: inefficient filtering of wastes from the blood
- hypoproteinemia: low blood protein
- edema: swelling in parts of the body
One or more of these symptoms can be the first sign of kidney disease. But how would you know, for example, whether you have proteinuria? Before seeing a doctor, you may not. But some of these symptoms have signs, or visible manifestations:
- Proteinuria may cause foamy urine.
- Blood may cause the urine to be pink or cola-colored.
- Edema may be obvious in hands and ankles, especially at the end of the day, or around the eyes when awakening in the morning, for example.
[Top]
How is glomerular disease diagnosed?
Patients with glomerular disease have significant amounts of protein in the urine, which may be referred to as "nephrotic range" if levels are very high. Red blood cells in the urine are a frequent finding as well, particularly in some forms of glomerular disease. Urinalysis provides information about kidney damage by indicating levels of protein and red blood cells in the urine. Blood tests measure the levels of waste products such as creatinine and urea nitrogen to determine whether the filtering capacity of the kidneys is impaired. If these lab tests indicate kidney damage, the doctor may recommend ultrasound or an x ray to see whether the shape or size of the kidneys is abnormal. These tests are called renal imaging. But since glomerular disease causes problems at the cellular level, the doctor will probably also recommend a kidney biopsy—a procedure in which a needle is used to extract small pieces of tissue for examination with different types of microscopes, each of which shows a different aspect of the tissue. A biopsy may be helpful in confirming glomerular disease and identifying the cause.
[Top]
What causes glomerular disease?
A number of different diseases can result in glomerular disease. It may be the direct result of an infection or a drug toxic to the kidneys, or it may result from a disease that affects the entire body, like diabetes or lupus. Many different kinds of diseases can cause swelling or scarring of the nephron or glomerulus. Sometimes glomerular disease is idiopathic, meaning that it occurs without an apparent associated disease.
The categories presented below can overlap: that is, a disease might belong to two or more of the categories. For example, diabetic nephropathy is a form of glomerular disease that can be placed in two categories: systemic diseases, since diabetes itself is a systemic disease, and sclerotic diseases, because the specific damage done to the kidneys is associated with scarring.
Autoimmune Diseases
When the body's immune system functions properly, it creates protein-like substances called antibodies and immunoglobulins to protect the body against invading organisms. In an autoimmune disease, the immune system creates autoantibodies, which are antibodies or immunoglobulins that attack the body itself. Autoimmune diseases may be systemic and affect many parts of the body, or they may affect only specific organs or regions.
Systemic lupus erythematosus (SLE) affects many parts of the body: primarily the skin and joints, but also the kidneys. Because women are more likely to develop SLE than men, some researchers believe that a sex-linked genetic factor may play a part in making a person susceptible, although viral infection has also been implicated as a triggering factor. Lupus nephritis is the name given to the kidney disease caused by SLE, and it occurs when autoantibodies form or are deposited in the glomeruli, causing inflammation. Ultimately, the inflammation may create scars that keep the kidneys from functioning properly. Conventional treatment for lupus nephritis includes a combination of two drugs, cyclophosphamide, a cytotoxic agent that suppresses the immune system, and prednisolone, a corticosteroid used to reduce inflammation. A newer immunosuppressant, mychophenolate mofetil (MMF), has been used instead of cyclophosphamide. Preliminary studies indicate that MMF may be as effective as cyclophosphamide and has milder side effects.
Goodpasture's Syndrome involves an autoantibody that specifically targets the kidneys and the lungs. Often, the first indication that patients have the autoantibody is when they cough up blood. But lung damage in Goodpasture's Syndrome is usually superficial compared with progressive and permanent damage to the kidneys. Goodpasture's Syndrome is a rare condition that affects mostly young men but also occurs in women, children, and older adults. Treatments include immunosuppressive drugs and a blood-cleaning therapy called plasmapheresis that removes the autoantibodies.
IgA nephropathy is a form of glomerular disease that results when immunoglobulin A (IgA) forms deposits in the glomeruli, where it creates inflammation. IgA nephropathy was not recognized as a cause of glomerular disease until the late 1960s, when sophisticated biopsy techniques were developed that could identify IgA deposits in kidney tissue.
The most common symptom of IgA nephropathy is blood in the urine, but it is often a silent disease that may go undetected for many years. The silent nature of the disease makes it difficult to determine how many people are in the early stages of IgA nephropathy, when specific medical tests are the only way to detect it. This disease is estimated to be the most common cause of primary glomerulonephritis—that is, glomerular disease not caused by a systemic disease like lupus or diabetes mellitus. It appears to affect men more than women. Although IgA nephropathy is found in all age groups, young people rarely display signs of kidney failure because the disease usually takes several years to progress to the stage where it causes detectable complications.
No treatment is recommended for early or mild cases of IgA nephropathy when the patient has normal blood pressure and less than 1 gram of protein in a 24-hour urine output. When proteinuria exceeds 1 gram/day, treatment is aimed at protecting kidney function by reducing proteinuria and controlling blood pressure. Blood pressure medicines—angiotensin—converting enzyme inhibitors (ACE inhibitors) or angiotensin receptor blockers (ARBs)—that block a hormone called angiotensin are most effective at achieving those two goals simultaneously.
Hereditary Nephritis—Alport Syndrome
The primary indicator of Alport syndrome is a family history of chronic glomerular disease, although it may also involve hearing or vision impairment. This syndrome affects both men and women, but men are more likely to experience chronic kidney disease and sensory loss. Men with Alport syndrome usually first show evidence of renal insufficiency while in their twenties and reach total kidney failure by age 40. Women rarely have significant renal impairment, and hearing loss may be so slight that it can be detected only through testing with special equipment. Usually men can pass the disease only to their daughters. Women can transmit the disease to either their sons or their daughters. Treatment focuses on controlling blood pressure to maintain kidney function.
Infection-related Glomerular Disease
Glomerular disease sometimes develops rapidly after an infection in other parts of the body. Acute post-streptococcal glomerulonephritis (PSGN) can occur after an episode of strep throat or, in rare cases, impetigo (a skin infection). The Streptococcus bacteria do not attack the kidney directly, but an infection may stimulate the immune system to overproduce antibodies, which are circulated in the blood and finally deposited in the glomeruli, causing damage. PSGN can bring on sudden symptoms of swelling (edema), reduced urine output (oliguria), and blood in the urine (hematuria). Tests will show large amounts of protein in the urine and elevated levels of creatinine and urea nitrogen in the blood, thus indicating reduced kidney function. High blood pressure frequently accompanies reduced kidney function in this disease.
PSGN is most common in children between the ages of 3 and 7, although it can strike at any age, and it most often affects boys. It lasts only a brief time and usually allows the kidneys to recover. In a few cases, however, kidney damage may be permanent, requiring dialysis or transplantation to replace renal function.
Bacterial endocarditis, infection of the tissues inside the heart, is also associated with subsequent glomerular disease. Researchers are not sure whether the renal lesions that form after a heart infection are caused entirely by the immune response or whether some other disease mechanism contributes to kidney damage. Treating the heart infection is the most effective way of minimizing kidney damage. Endocarditis sometimes produces chronic kidney disease (CKD).
HIV, the virus that leads to AIDS, can also cause glomerular disease. Between 5 and 10 percent of people with HIV experience kidney failure, even before developing full-blown AIDS. HIV-associated nephropathy usually begins with heavy proteinuria and progresses rapidly (within a year of detection) to total kidney failure. Researchers are looking for therapies that can slow down or reverse this rapid deterioration of renal function, but some possible solutions involving immunosuppression are risky because of the patients' already compromised immune system.
Sclerotic Diseases
Glomerulosclerosis is scarring (sclerosis) of the glomeruli. In several sclerotic conditions, a systemic disease like lupus or diabetes is responsible. Glomerulosclerosis is caused by the activation of glomerular cells to produce scar material. This may be stimulated by molecules called growth factors, which may be made by glomerular cells themselves or may be brought to the glomerulus by the circulating blood that enters the glomerular filter.
Diabetic nephropathy is the leading cause of glomerular disease and of total kidney failure in the United States. Kidney disease is one of several problems caused by elevated levels of blood glucose, the central feature of diabetes. In addition to scarring the kidney, elevated glucose levels appear to increase the speed of blood flow into the kidney, putting a strain on the filtering glomeruli and raising blood pressure.
Diabetic nephropathy usually takes many years to develop. People with diabetes can slow down damage to their kidneys by controlling their blood glucose through healthy eating with moderate protein intake, physical activity, and medications. People with diabetes should also be careful to keep their blood pressure at a level below 140/90 mm Hg, if possible. Blood pressure medications called ACE inhibitors and ARBs are particularly effective at minimizing kidney damage and are now frequently prescribed to control blood pressure in patients with diabetes and in patients with many forms of kidney disease.
Focal segmental glomerulosclerosis (FSGS) describes scarring in scattered regions of the kidney, typically limited to one part of the glomerulus and to a minority of glomeruli in the affected region. FSGS may result from a systemic disorder or it may develop as an idiopathic kidney disease, without a known cause. Proteinuria is the most common symptom of FSGS, but, since proteinuria is associated with several other kidney conditions, the doctor cannot diagnose FSGS on the basis of proteinuria alone. Biopsy may confirm the presence of glomerular scarring if the tissue is taken from the affected section of the kidney. But finding the affected section is a matter of chance, especially early in the disease process, when lesions may be scattered.
Confirming a diagnosis of FSGS may require repeat kidney biopsies. Arriving at a diagnosis of idiopathic FSGS requires the identification of focal scarring and the elimination of possible systemic causes such as diabetes or an immune response to infection. Since idiopathic FSGS is, by definition, of unknown cause, it is difficult to treat. No universal remedy has been found, and most patients with FSGS progress to total kidney failure over 5 to 20 years. Some patients with an aggressive form of FSGS reach total kidney failure in 2 to 3 years. Treatments involving steroids or other immunosuppressive drugs appear to help some patients by decreasing proteinuria and improving kidney function. But these treatments are beneficial to only a minority of those in whom they are tried, and some patients experience even poorer kidney function as a result. ACE inhibitors and ARBs may also be used in FSGS to decrease proteinuria. Treatment should focus on controlling blood pressure and blood cholesterol levels, factors that may contribute to kidney scarring.
Other Glomerular Diseases
Membranous nephropathy, also called membranous glomerulopathy, is the second most common cause of the nephrotic syndrome (proteinuria, edema, high cholesterol) in U.S. adults after diabetic nephropathy. Diagnosis of membranous nephropathy requires a kidney biopsy, which reveals unusual deposits of immunoglobulin G and complement C3, substances created by the body's immune system. Fully 75 percent of cases are idiopathic, which means that the cause of the disease is unknown. The remaining 25 percent of cases are the result of other diseases like systemic lupus erythematosus, hepatitis B or C infection, or some forms of cancer. Drug therapies involving penicillamine, gold, or captopril have also been associated with membranous nephropathy. About 20 to 40 percent of patients with membranous nephropathy progress, usually over decades, to total kidney failure, but most patients experience either complete remission or continued symptoms without progressive kidney failure. Doctors disagree about how aggressively to treat this condition, since about 20 percent of patients recover without treatment. ACE inhibitors and ARBs are generally used to reduce proteinuria. Additional medication to control high blood pressure and edema is frequently required. Some patients benefit from steroids, but this treatment does not work for everyone. Additional immunosuppressive medications are helpful for some patients with progressive disease.
Minimal change disease (MCD) is the diagnosis given when a patient has the nephrotic syndrome and the kidney biopsy reveals little or no change to the structure of glomeruli or surrounding tissues when examined by a light microscope. Tiny drops of a fatty substance called a lipid may be present, but no scarring has taken place within the kidney. MCD may occur at any age, but it is most common in childhood. A small percentage of patients with idiopathic nephrotic syndrome do not respond to steroid therapy. For these patients, the doctor may recommend a low-sodium diet and prescribe a diuretic to control edema. The doctor may recommend the use of nonsteroidal anti-inflammatory drugs to reduce proteinuria. ACE inhibitors and ARBs have also been used to reduce proteinuria in patients with steroid-resistant MCD. These patients may respond to larger doses of steroids, more prolonged use of steroids, or steroids in combination with immunosuppressant drugs, such as chlorambucil, cyclophosphamide, or cyclosporine.
[Top]
What are renal failure and end-stage renal disease?
Renal failure is any acute or chronic loss of kidney function and is the term used when some kidney function remains. Total kidney failure, sometimes called end-stage renal disease (ESRD), indicates permanent loss of kidney function. Depending on the form of glomerular disease, renal function may be lost in a matter of days or weeks or may deteriorate slowly and gradually over the course of decades.
Acute Renal Failure
A few forms of glomerular disease cause very rapid deterioration of kidney function. For example, PSGN can cause severe symptoms (hematuria, proteinuria, edema) within 2 to 3 weeks after a sore throat or skin infection develops. The patient may temporarily require dialysis to replace renal function. This rapid loss of kidney function is called acute renal failure (ARF). Although ARF can be life-threatening while it lasts, kidney function usually returns after the cause of the kidney failure has been treated. In many patients, ARF is not associated with any permanent damage. However, some patients may recover from ARF and subsequently develop CKD.
Chronic Kidney Disease
Most forms of glomerular disease develop gradually, often causing no symptoms for many years. CKD is the slow, gradual loss of kidney function. Some forms of CKD can be controlled or slowed down. For example, diabetic nephropathy can be delayed by tightly controlling blood glucose levels and using ACE inhibitors and ARBs to reduce proteinuria and control blood pressure. But CKD cannot be cured. Partial loss of renal function means that some portion of the patient's nephrons have been scarred, and scarred nephrons cannot be repaired. In many cases, CKD leads to total kidney failure.
Total Kidney Failure
To stay alive, a patient with total kidney failure must go on dialysis—hemodialysis or peritoneal dialysis—or receive a new kidney through transplantation. Patients with CKD who are approaching total kidney failure should learn as much about their treatment options as possible so they can make an informed decision when the time comes. With the help of dialysis or transplantation, many people continue to lead full, productive lives after reaching total kidney failure.
[Top]
Points to Remember
- The kidneys filter waste and extra fluid from the blood.
- The filtering process takes place in the nephron, where microscopic blood vessel filters, called glomeruli, are attached to fluid-collecting tubules.
- A number of different disease processes can damage the glomeruli and thereby cause kidney failure. Glomerulonephritis and glomerulosclerosis are broad terms that include many forms of damage to the glomeruli.
- Some forms of kidney failure can be slowed down, but scarred glomeruli can never be repaired.
- Treatment for the early stages of kidney failure depends on the disease causing the damage.
- Early signs of kidney failure include blood or protein in the urine and swelling in the hands, feet, abdomen, or face. Kidney failure may be silent for many years.
The Nephrotic Syndrome
- The nephrotic syndrome is a condition marked by very high levels of protein in the urine; low levels of protein in the blood; swelling, especially around the eyes, feet, and hands; and high cholesterol.
- The nephrotic syndrome is a set of symptoms, not a disease in itself. It can occur with many diseases, so prevention relies on controlling the diseases that cause it.
- Treatment of the nephrotic syndrome focuses on identifying and treating the underlying cause, if possible, and reducing high cholesterol, blood pressure, and protein in the urine through diet, medication, or both.
- The nephrotic syndrome may go away once the underlying cause, if known, is treated. However, often a kidney disease is the underlying cause and cannot be cured. In these cases, the kidneys may gradually lose their ability to filter wastes and excess water from the blood. If kidney failure occurs, the patient will need to be on dialysis or have a kidney transplant.
[Top]
Definitions
Signs and Symptoms of Glomerulonephritis
edema (eh-DEE-muh): Swelling caused by the accumulation of fluid in cells and tissues. In kidney failure, fluid may collect in the feet, hands, abdomen, or face.
hematuria (HEE-muh-TOOR-ee-uh): Blood in the urine. Blood may turn the urine pink or cola-colored.
hypoproteinemia (HY-po-PRO-teen-EE-mee-uh): Reduced levels of protein in the blood.
proteinuria (PRO-tee-NOOR-ee-uh): Large amounts of protein in the urine.
uremia (yoo-REE-mee-uh): Accumulation of urea and other wastes in the blood. These wastes, which become toxic in large amounts, are normally eliminated through urination.
Diseases and Conditions
autoimmune (AW-toh-ih-MYOON) disease: A disease in which the body's own disease-fighting cells attack the body itself.
hypertension (HY-per-TEN-shun): High blood pressure, a condition that can cause kidney damage or be caused by kidney disease.
idiopathic (id-ee-o-PATH-ik) disease: A disease that occurs without a known cause.
nephrotoxic (NEF-ro-TOKS-ik): Damaging to the kidneys.
sclerotic (skleh-ROT-ik) disease: A disease in which tissues become hardened or scarred.
systemic (sis-TEM-ik) disease: A disease that affects multiple parts of the body, often as a result of substances circulating in the blood.
Treatments and Procedures
biopsy (BY-op-see): A procedure in which a needle is used to obtain small pieces of tissue from an organ for examination under different types of microscopes, each of which shows a different aspect of the tissue.
dialysis (dy-AL-ih-sis): A medical treatment that removes wastes and extra fluid from the blood after the kidneys have stopped working.
immunosuppressant (im-YOON-oh-suh-PRESS-unt): A medicine given to block the body's immune system.
plasmapheresis (PLAZ-muh-fer-EE-sis): A medical treatment in which the blood is treated outside the body to remove harmful antibodies, and then returned to the patient.
Kidney Parts and Organic Substances
antibody (AN-tee-BOD-ee): A molecule that protects the body against disease by attacking foreign tissues or organisms. Antibodies are also called immunoglobulins.
antigen (AN-tih-jen): A substance that triggers a response from the body's immune system.
autoantibody (AW-toh-AN-tee-bod-ee): An antibody that attacks the body itself.
creatinine (kree-AT-ih-nin): A waste product in the blood that results from the normal breakdown of muscle. Healthy kidneys filter creatinine from the blood.
glomerulus (gloh-MEHR-yoo-lus): The tiny cluster of looping blood vessels in the nephron, where wastes are filtered from the blood.
lipid (LIP-id): One of several fatty substances used in cells. Excess lipids in the blood may result in harmful deposits in blood vessels.
nephron (NEF-rahn): One of a million tiny filtering units in each kidney. Each nephron is made up of both a glomerulus and a fluid-collecting tubule that processes extra water and wastes.
protein (PRO-teen): A substance found in food and used by the body to grow, repair tissue, and fight disease.
urea (yoo-REE-uh): A waste material found in blood after protein has been broken down. Healthy kidneys remove urea from the blood. Damaged kidneys may allow urea to accumulate in the blood, thus causing uremia.
[Top]
This content is provided as a service of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), part of the National Institutes of Health. The NIDDK translates and disseminates research findings through its clearinghouses and education programs to increase knowledge and understanding about health and disease among patients, health professionals, and the public. Content produced by the NIDDK is carefully reviewed by NIDDK scientists and other experts.
This information is not copyrighted. The NIDDK encourages people to share this content freely.
[Top]
April 2014